


Infant Deaths - Is there an Association with Vaccines?
By Julian Gillespie, LLB, BJuris

Shared with Permission - there will be more information relating to SIDS and vaccination in the coming days.

For over a decade, medical researchers Neil Miller and Gary Goldman have been looking at links between infant vaccines and Infant Mortality Rates, or IMR, becoming specialists on the subject since first examining IMR data from 34 countries back in 2011.

In their 2011 peer-reviewed science paper, they were able to show and conclude:
The infant mortality rate (IMR) is one of the most important indicators of the socio-economic well-being and public health conditions of a country. The US childhood immunization schedule specifies 26 vaccine doses for infants aged less than 1 year—the most in the world—yet 33 nations have lower IMRs.
Linear regression analysis of unweighted mean IMRs showed a high statistically significant correlation between increasing number of vaccine doses and increasing infant mortality rates.
The simple meaning from these findings is that the data strongly suggests increased doses of childhood vaccines lead to higher rates of infant death.
Miller and Goldman were concerned with the data they were analysing and undertook a further study published in 2012, where again the association between increased numbers of childhood vaccines and hospitalisations, or even death, was statistically significant. They concluded:
Our findings show a positive correlation between the number of vaccine doses administered and the percentage of hospitalizations and deaths. Since vaccines are given to millions of infants annually, it is imperative that health authorities have scientific data from synergistic toxicity studies on all combinations of vaccines that infants might receive. Finding ways to increase vaccine safety should be the highest priority.
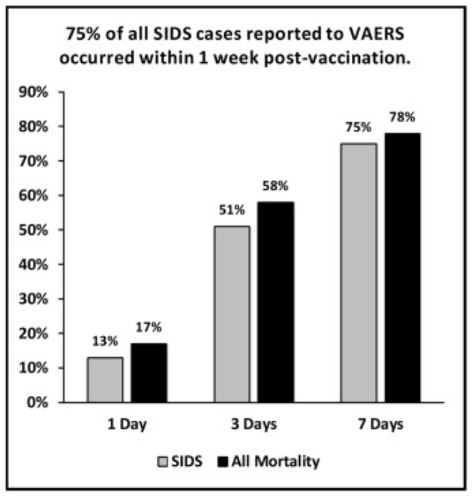
Then in 2021 Miller had another study published looking at Sudden Infant Deaths (SIDS), where he examined the US Vaccine Adverse Event Reporting System (VAERS), then closely surveyed the medical literature discussing SIDS going back to the early 1900s. The data was again showing a statistically significant association between SIDS and infants receiving a vaccine. The VAERS analysis demonstrated that 75% of SIDS cases arose within 7 days of receiving a vaccine. Miller stated:
The findings in this study revealed that infant deaths and SIDS cases were not randomly distributed each day. Instead, infant mortality and SIDS cases reported to VAERS tended to occur in temporal proximity to vaccine administration, that is, they clustered in the early post-vaccination period—Day 1 through Day 7.
Surveying the medical literature of the 1900s Miller discovered some telling studies. One included the work of Australian physician Archie Kalokerinos in 1974, who questioned why 1 in 2 aboriginal babies in the 1960s and 1970s were succumbing to unexplained death. Miller noted that Dr Kalokerinos had:
.. realized the deaths were occurring shortly after the babies were vaccinated. Health officials had recently initiated a mass vaccination campaign to protect Aborigine babies; their deaths corresponded with the vaccination program. Kalokerinos realized that these babies were severely malnourished. Their undeveloped immune systems couldn't handle the additional stress of vaccination.
In 1974 Dr Kalokerinos observed:
"Some would die within hours from acute vitamin C deficiency precipitated by the immunization. Others would suffer immunological insults and die later from pneumonia, gastroenteritis, or malnutrition."
In the foreword to the book by Dr Kalokerinos titled Every Second Child, Linus Pauling who won the Nobel Prize in chemistry remarked:
I believe that the conclusion reached by Dr. Kalokerinos that the high infant mortality and generally high incidence of disease among the Aboriginal infants are to be attributed in considerable part to a low body content of vitamin C is correct. Moreover, it seems to be not unlikely that the Australian Aborigines have a special immunological problem, as described by Dr. Kalokerinos, and that in addition the deficiency in vitamin C is exacerbated by immunizations and inoculations, since it is known that immunization and inoculation lead to destruction of vitamin C. Dr. Kalokerinos deserves much credit for having made these discoveries.
Japanese authorities were quick to notice the work of Dr Kalokerinos. In a telling move which appeared to demonstrate that Australian Aboriginal babies were not alone in being susceptible to post-vaccine death, Japanese authorities in 1975 raised the age for receiving vaccines from 3 months to 2 years. After reviewing the Japanese data Miller summarised the effect:
In addition, from the early 1970s (a period when 3-month-old infants were vaccinated) to the mid-1980s (ten years after the age of vaccination was raised to 2 years) the Japanese infant mortality rate (infant deaths per 1000 live births) declined from 12.4–5.0 — a 60 % improvement.
Japanese authorities concluded in the late 1980s:
It is clear that delaying the initial vaccination until a child is 24 months, regardless of the type of vaccine, reduces most of the temporally associated severe adverse reactions.
Miller then reviewed a number of reports of SIDS in the US seemingly associated with the DPT vaccine, the combination vaccine for diphtheria, tetanus, and pertussis. Despite poor investigations by the US CDC which sought to deem of string of SIDS deaths soon after DPT vaccination as 'coincidental', Miller preferred the more thorough 1982 study by Dr William Torch which 'found that unvaccinated babies who died from SIDS did so most often in the fall or winter while vaccinated babies died most often at 2 and 4 months—the same ages when initial doses of DPT were given to infants'. Dr William Torch concluded:
DPT may be a generally unrecognized major cause of sudden infant and early childhood death, and the risks of immunization may outweigh its potential benefits. A need for re-evaluation and possible modification of current vaccination procedures is indicated by this study.

Miller did not stop with the DPT vaccine. He then looked at the hexavalent (6-in-1) vaccine, and especially a confidential 2011 report created by one of the manufacturers, GlaxoSmithKline (GSK), which had been made available by an Italian court. Again the data was compelling and damning. Miller noted:
However, despite the manufacturer's conclusion that its hexavalent vaccine does not increase the risk of sudden death, Table 36 on page 249 of the confidential report shows that 62.7% of these deaths clustered within 3 days post-vaccination and 89.6% occurred within 7 days post-vaccination. Perhaps more significantly, 97% (65 of the 67 reported infant deaths) occurred in the first 10 days post-vaccination while just 3% (2 of the 67 infant deaths) occurred in the next 10 days.
Pushing on Miller reviewed even more papers and studies looking at different regions, and a trend of the same post-vaccination sudden infant death became clear. In a 2011 study by Kuhnert and colleagues, they found evidence of a 16-fold increased risk of sudden unexpected death following the fourth dose of a pentavalent (5-in-1) or hexavalent (6-in-1) vaccine.
Miller then turned to a 2014 study by Matturri and his colleagues, noting the authors examined:
13 sudden infant deaths that occurred within 7 days of a hexavalent vaccine. Histological analyses of the brainstem and cerebellum revealed brain edema [swelling of the brain] and congestion in all victims.
Throughout the review paper by Miller is seen study after study by respected scientists evidencing again and again a strong correlation of SIDS cases within 7-10 days of receiving any one of a variety of childhood vaccines.
In reviewing a 2015 CDC report produced by Moro and colleagues analysing VAERS death reports between 1997 and 2013, Miller was able to again to show this trend in the data between the date of receipt of a childhood vaccine, and reported SIDS cases :
The most common cause of death among 1244 child reports with autopsy findings or death certificates available for review was SIDS. Most SIDS cases were among infants 2–4 months of age. Among the 1165 infant reports, 86.2% received multiple vaccines prior to death. The median onset interval, the period from vaccination to death, was 2 days. SIDS reports were most common among children who had received DTaP, hepatitis B, inactivated polio, Hib, and pneumococcal vaccines simultaneously prior to death.
By the end of his review Miller provided readers with a stark conclusion:
This study found that a substantial proportion of infant deaths and SIDS cases occurred in temporal proximity to vaccine administration. The excess of deaths during these early post-vaccination periods was statistically significant (p < 0.00001).
With such compelling data being shown in countless studies around the world, Miller and Goldman collaborated once again to produce two further studies published in 2023.
Paper #1
The title to their first paper in February 2023 saw them returning to their roots, bringing in updated data to show their ground-breaking 2011 study (above) had only been further confirmed with the passage of time:
Reaffirming a Positive Correlation Between Number of Vaccine Doses and Infant Mortality Rates: A Response to Critics
Miller and Goldman wrote the February 2023 paper in order to answer critics of their 2011 paper, that the two should have included all 185 nations in their study. Those critics tried analysing all 185 nations with results that appeared to refute and discredit the 2011 findings showing a link between increased vaccines received, and an increase in Infant Mortality Rates.
But as Miller and Goldman were able to show in this study, their critics had used old data, and they had used data from countries that were very dissimilar, particularly from countries known to have high Infant Mortality Rates due to significant malnutrition, underdeveloped sewerage and sanitation systems, poverty, and substandard healthcare systems. These essentially Third World problems confound or skew statistical analysis, meaning it becomes much more difficult to analyse whether Infant deaths are due more likely to vaccines, or if one of these other threats to childhood health and life, like we all know bad sewerage and malnutrition represent, could be the cause of death. These confounding factors helped their critics to essentially take advantage of other causes of death to reduce the appearance of vaccines as the likely cause of infant deaths.
Immediately Miller and Goldman were able to show their critics had used questionable statistical methods for trying to challenge their 2011 study. That called into questions the motivations of their critics by using flawed techniques. But to put the debate beyond any further question, the two scientists went one better by collecting country data that specifically excluded nations with confounding problems (poverty, sanitations problems etc), and where their 2011 study looked at 30 nations, in this updated study they included the latest 2019 data from the UNICEF Date Warehouse for 44 nations with very similar standards of living in respect of children - in other words, countries with uniformity in socioeconomic factors - a critical common baseline for comparing apples with apples. They also used up-to-date data from the World Health Organization, the European Centre for Disease Prevention and Control, and national governments.
This study was therefore much stronger than their first in 2011, using a wide collection of up-to-date data their critics chose to intentionally not include in their flawed analysis.
And their 2011 results were only reaffirmed and reconfirmed and strengthened: increased vaccine doses result in a country having an increased Infant Mortality Rate .. meaning more infant deaths.
Figure 4 from the study makes it plain to see - the more vaccine doses received along the x-axis increases the number of deaths on the y-axis:

In light of such comprehensive findings secured with greater certainty with the passage of time and improved data sets, Miller and Goldman were able to confidently conclude, after having exposed the very cynical and questionable efforts of their critics:
There is a positive correlation between infant vaccines and infant mortality rates. This relationship is most pronounced in analyses of the most highly developed homogenous nations ..
Health authorities in all nations have an obligation to determine whether their immunization schedules are achieving desired goals.
Paper #2
The title to their second paper in July 2023 clearly details the breadth of their research:
Neonatal, Infant, and Under Age Five Vaccine Doses Routinely Given in Developed Nations and Their Association With Mortality Rates
Critically, this study examined 50 nations with differing vaccine doses administered to neonates/newborns (<28days); compared to the number of doses administered to babies under 1 year of age; compared to the number of doses administered to infants under 5 years. Their statistical analysis produced results for three categories: Neonatal Mortality Rates (NMRs), Infant Mortality Rates (IMRs), and Under Aged 5 Mortality Rates (U5MRs).
The results discovered by Miller and Goldman suggest only real risks to neonates and infants from early vaccinations:
Approximately 45-75% of all infant deaths and 30-60% of underage five deaths occur during the neonatal period [the first 4 weeks of life].
About 75% of neonatal deaths occur during the first week of life, the same time period when the birth doses of required neonatal vaccines are administered.
The mortality rate for vaccinated infants less than 6 months of age was significantly higher than that of vaccinated infants 6 months to 1 year of age.
One-third (33.3%) of premature infants vaccinated at 70 days of age or less had major adverse reactions compared with none when vaccinated over 70 days of age.
Vaccinated infants born prematurely were five times (5x) more likely to be diagnosed with a neurodevelopmental disorder than vaccinated non-preterm children, and 14 times more likely when compared to children who were born full term and not vaccinated.
With the above data Miller and Goldman then reviewed other studies to make some further compelling observations:
Studies provide evidence that premature newborns (and full-term babies with low birth weight) may be particularly susceptible to serious adverse reactions to vaccines, including life-threatening apnea. Sánchez et al. found that 12% of vaccinated preterm infants experienced apnea within 72 hours post-vaccination. Preterm infants who were vaccinated at a lower weight had the most severe cases. Apnea preceding sudden death has been well-documented.
Seeking to further understand the adverse risk data revealed in their findings, Miller and Goldman reviewed the study by DeMeo and colleagues from which they observed:
Low birth weight infants were significantly more likely to develop sepsis, and require respiratory support and intubation in the three days post-vaccination compared to the three days prior to vaccination.
After reviewing the study by Pourcyrous and colleagues they further observed:
When premature infants were given more than one vaccine concurrently, they were four times more likely to have adverse cardiorespiratory events (apnea, bradycardia, or oxygen desaturation) .. compared to preterm infants who received a single vaccine.
These reviews of earlier studies then allowed Miller and Goldman to make a critical statement:
These studies indicate that some deaths attributed to preterm birth or low birth weight may be associated with the hepatitis B and/or BCG vaccines administered at birth, and the true cause of these deaths could be misclassified.
Reminiscent of the Japanese experience described above, (after Japan raised the age for receiving first vaccines from 3 months to 2 years), Miller and Goldman found their statistical analysis of the 50 nation data lead them to reason:
Our hypothesis is that the additional doses administered from the second through fifth years of life have less effect on under age five mortality than vaccines administered earlier in life.
This statement by implication suggests vaccines administered to infants less than 2 years pose the greatest risk of death to infants and neonates. And the logic behind this hypothesis is pretty easy to understand drawing from their earlier 2011 study, namely, it is all about body mass:
Children in the first year of life, as compared to the second through fifth years of life, weigh less and are receiving more vaccines in a shorter time period. Receipt of vaccines at a younger age (associated with lower weight), and multiple vaccines administered concurrently (as regularly occurs during infancy), have been shown to increase the risk of hospitalizations and death.
That is, infants aged 2, 3, 4, or 5 years are considerably more developed compared to a neonate of less than 4 weeks, particularly in their ability to withstand the immune system shock induced by vaccines and their synthetic inflammatory adjuvants. In other words, a baby 2 weeks old given the same dose as would be given to a 3 year old, well, that 2 week old body is simply not strong enough to overcome the induced shock, leading by implication from the data put forward by Miller and Goldman, to many an infant succumbing to death in the days after. And when multiple vaccines are administered one after the other, then the shock is only greater, thereby increasing the likelihood of an adverse outcome or even death.
On this point Professor Robyn Cosford further observed after reviewing this essay:
The exaggerated effect in the under 2 year-olds is not only due to the dose/weight issue but also importantly that the younger the infant, the more immature the detox mechanisms, the nervous system, and the immune system and hence, the less likely the child is to be able to safely protect itself against effects [immune system shocks induced by vaccines], on the developing brain in particular.
Referring back to their 2011 study on the top 30 nations, (infant vaccine doses ranging from 12 to 26), and the data appears to clearly prove their point, namely, the Infant Mortality Rate increased by a factor of 0.167 deaths for every 1,000 births with each additional vaccine required under a nation's vaccine schedule. Equally, for every reduction of six vaccines said to be required, (26 to 20 to 14 etc), one baby per 1,000 births was saved.
An even more stark statistic for neonates (under 4 weeks old) found a mean Infant Mortality Rate of 2.87 in those babies not required to receive any vaccines, and an Infant Mortality Rate of 4.15 in those neonates receiving two vaccines. That represents a 44.6% increase in neonate deaths between the unvaccinated and the vaccinated, which should be an alarming safety signal for all parents, and governments asserting the safety of these unnatural products.
By the end of this critical and enlightening study Miller and Goldman were able to confidently conclude:
There are statistically significant positive correlations between neonatal, infant, and under age five mortality rates of developed nations and the number of early childhood vaccine doses that are routinely given.
When developed nations require two versus zero neonatal vaccine doses, or many versus fewer infant vaccine doses, our study suggests there may be unintended consequences that increase all-cause mortality.
In words we can all understand the work of Miller and Goldman puts 'the writing on the wall'. Whether neonates or infants or under 5 years, any number of vaccines are shown to positively correlate with increased all-cause mortality, being just another science term for death. Neonates receiving vaccines are clearly at most risk. That risk appears to statistically decrease when vaccines are started only from 2 years, but the risk of death is never eliminated.
Where death does not occur, then the next relevant question becomes: did those vaccines nonetheless do any harm to the child?
That question moves us in the direction of controversial subjects like Autism and a range of childhood illnesses seen now that once upon time our children never experienced, so what has happened?
Fortunately, the data on those subjects has started to become clear enough for all to understand, where it can be briefly stated, childhood vaccines are not coming out on top as winners .. but rather being found to maybe protect against certain intended disease, but at the cost of inviting in for life, many others.

Julian Gillespie is a lawyer and former barrister in Australia, known for his Covid-19 research and advocacy. His work includes seeking to have the provisional approval of Covid-19 vaccines declared legally invalid due to failures to meet regulatory standards. Julian is also a director of Children's Health Defense, Australia.

No words.
Only Fury.
Thank you for this information 🙏 I will be printing it out and sharing everywhere I can.